- Table of Contents
- Introduction
- 1- What Is Healthcare Quality Improvement?
- 2- Why Quality Improvement Matters: The Scale of the Problem
- 3- The Plan-Do-Study-Act (PDSA) Cycle
- 4- Total Quality Management (TQM) in Healthcare
- 5- Lean Methodology in Healthcare
- 6- Six Sigma in Healthcare
- 7- Lean Six Sigma: A Combined Approach
- 8- ISO Standards and Quality Management Systems in Healthcare
- 9- Applying Quality Improvement in Public Health and NGO Settings
- 10- Building a Culture of Quality: The Human Dimension
- 11- Measurement and Data in Quality Improvement
- 12 - Challenges and Limitations of Quality Improvement Methodologies
- 13 - Selecting the Right Methodology for Your Context
- Conclusion
Introduction
Healthcare quality improvement is one of the most pressing concerns facing health systems across the world. Whether in a busy urban hospital, a district health centre, a non-governmental organisation running field clinics, or a public health ministry designing national policy, the need to deliver safe, effective, and patient-centred care consistently is universal. Yet the gap between what we know and what we deliver remains stubbornly wide. Practices vary between institutions and countries, preventable harm continues to occur, and the resources available to act are frequently limited, unevenly distributed, or poorly coordinated.
Quality improvement in healthcare is not a single method or a one-off exercise. It is a structured, ongoing commitment to examining how care is delivered and making deliberate, evidence-informed changes to make it better. Across the field, a number of methodologies have emerged that provide practical tools, conceptual frameworks, and measurable processes to support that commitment. These include the Plan-Do-Study-Act cycle, Total Quality Management, Lean thinking, Six Sigma, and international standards such as the ISO 9001 framework. Each has distinct origins, strengths, and areas of application. Together, they form a toolkit that healthcare organisations can draw on depending on their context, capacity, and goals.
1- What Is Healthcare Quality Improvement?
Healthcare quality improvement refers to a systematic approach to enhancing the safety, effectiveness, efficiency, equity, and patient-centredness of healthcare services. It draws on data, structured methods, and collaborative action to identify gaps in care and implement changes that address them. Unlike audit, which primarily measures performance against standards, quality improvement is specifically oriented towards change. It asks not only whether care meets a standard but also how care can be actively redesigned to meet it more consistently.
The World Health Organisation frames quality of care around six dimensions: safety, effectiveness, efficiency, accessibility, acceptability, and equity. These dimensions apply as much to a field health post managed by an NGO in a conflict-affected region as they do to a tertiary hospital in a high-income country. The methodologies discussed in this article provide structured ways to work across all six dimensions, albeit with different emphases and tools.
Quality improvement also differs from research in important ways. Research aims to generate new knowledge through controlled study. Quality improvement aims to apply existing knowledge to improve local practice. It is iterative, context-sensitive, and dependent on frontline staff and patients as active participants rather than subjects. This distinction matters because it shapes how improvement work is designed, implemented, and evaluated.
2- Why Quality Improvement Matters: The Scale of the Problem
The case for systematic quality improvement rests on compelling evidence that current healthcare delivery, even in well-resourced settings, causes substantial preventable harm. According to the WHO Global Patient Safety Report 2024, more than one in ten patients experiences harm in medical care settings, and approximately half of that harm is considered preventable. The same report notes that globally, 1 in 20 patients suffers from preventable medication harm, with over half of this harm arising at the prescribing stage.
In low- and middle-income countries, the situation is particularly acute. The Agency for Healthcare Research and Quality notes that quality improvement is essential to achieving the triple aim of improving population health, enhancing patient experiences and outcomes, and reducing the per capita cost of care. Yet in many contexts where NGOs and public health organisations operate, basic infrastructure for quality systems, including data collection tools, trained improvement leads, and governance structures, is either absent or fragile. This means that simple, adaptable methodologies are not merely preferable but essential.
The financial case for improvement is equally strong. The WHO report notes that effective patient safety interventions, such as the Surgical Safety Checklist and strategies to prevent healthcare-associated infections, offer high returns on investment, demonstrating that targeted quality improvement efforts are not only medically beneficial but also economically sound. This matters for budget-constrained systems in both the public and NGO sectors, where every investment must be justified against competing priorities.
3- The Plan-Do-Study-Act (PDSA) Cycle
The Plan-Do-Study-Act cycle is one of the most widely used quality improvement frameworks in healthcare. Rooted in the work of W. Edwards Deming and the earlier scientific management principles of Walter Shewhart, the PDSA cycle provides a structured iterative method for testing change ideas on a small scale before implementing them more broadly. It is deliberately simple, making it accessible to clinical teams, community health workers, and NGO field staff without requiring specialist statistical knowledge.
The four stages of the cycle each have a distinct purpose. In the Plan phase, the improvement team identifies a specific problem, sets a measurable objective, designs a small-scale test of change, and predicts what the outcome will be. This prediction is important because it forces the team to make their assumptions explicit, which makes the Study phase more rigorous. In the Do phase, the team carries out the planned test, collects data, and documents observations, including any unexpected events or deviations from the plan. In the Study phase, the team analyses the data, compares the results to the predictions made in the Plan phase, and draws conclusions about whether the change produced the intended effect. In the Act phase, the team decides whether to adopt the change and scale it up, adapt it based on what was learned and run another cycle, or abandon it and try a different approach.
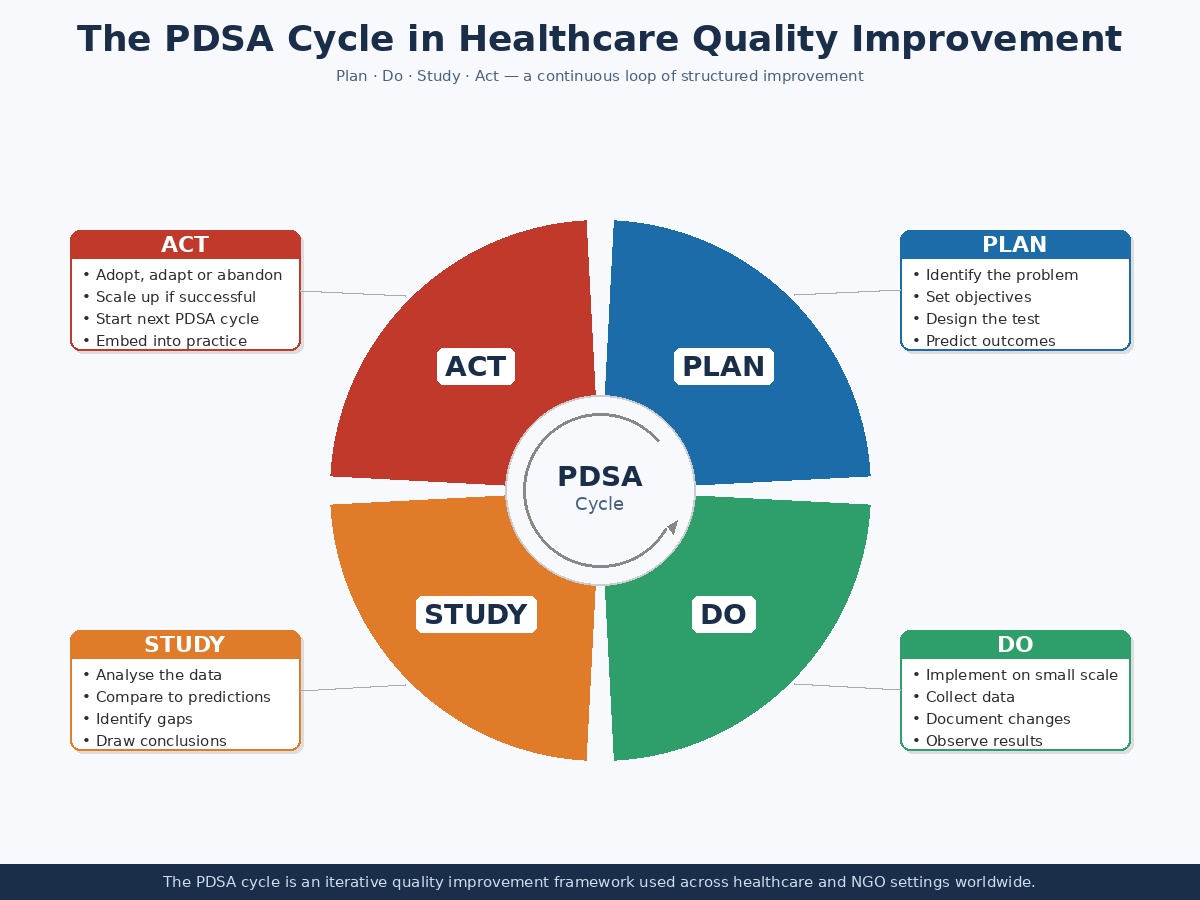
The power of the PDSA model lies in its iterative nature. No single cycle is expected to produce a perfect solution. Rather, each cycle generates learning that informs the next, building improvement progressively and reducing the risk of large-scale failure. This is particularly valuable in resource-limited settings where failed large interventions can have serious consequences for both patients and organisational credibility. In humanitarian health contexts, PDSA cycles are increasingly used to improve vaccination coverage, reduce medication errors, and strengthen referral pathways, often within weeks rather than months.

This advanced course provides a comprehensive exploration of strategic leadership in healthcare. Participants will gain insights into effective leadership strategies, learn to navigate complex healthcare environments, and develop the skills needed to drive organisational success. The course combines theoretical knowledge with practical applications, preparing healthcare professionals to become
4- Total Quality Management (TQM) in Healthcare
Total Quality Management is a comprehensive management philosophy that embeds quality into every aspect of an organisation rather than treating it as the responsibility of a single department or team. Developed from the work of quality theorists including Deming, Joseph Juran, and Philip Crosby, TQM became influential in manufacturing in the 1980s before being adopted widely across service industries, including healthcare. Its core principle is that quality is not inspected into a product or service after the fact but is designed and built in from the beginning through the involvement of every employee at every level.
In a healthcare setting, TQM translates into a sustained organisational commitment to continuous improvement, customer focus, process thinking, data-based decision-making, and employee empowerment. The customer in this context is primarily the patient, but TQM also recognises internal customers: the clinician depends on the laboratory, the laboratory depends on the procurement team, and so on. Improving quality therefore requires coordinating improvement across the entire chain of processes that contribute to patient care, not just in those areas that are most visible or most easily measured.
TQM in healthcare typically involves a number of interconnected activities. These include defining quality standards and aligning them with patient needs, mapping and analysing care processes to identify variation and waste, training staff in quality tools and improvement thinking, establishing measurement systems that track performance over time, creating feedback loops between management and frontline staff, and building a culture in which raising concerns and proposing improvements is expected and rewarded rather than discouraged.
TQM Principle | Application in Healthcare | Example |
| Customer focus | Centering care on patient needs and experience | Patient satisfaction surveys informing ward redesign |
| Employee involvement | Engaging frontline staff in improvement decisions | Nursing staff leading medication error reduction teams |
| Process approach | Treating care delivery as a system of linked processes | Mapping the patient journey from admission to discharge |
| Continuous improvement | Regular review and incremental enhancement of care | Monthly PDSA cycles on discharge planning |
| Evidence-based decisions | Using data to guide action rather than assumption | Using infection rates to target hand hygiene interventions |
| Leadership commitment | Senior management visibly driving quality culture | Executive-sponsored patient safety rounds |
TQM is most effective when it becomes genuinely embedded in organisational culture rather than sitting as a parallel structure or a set of compliance requirements. This is one of the most challenging aspects of implementing TQM in healthcare, where professional hierarchies, time pressures, and fragmented accountability structures can all work against the collaborative, cross-functional spirit that TQM requires. Research consistently shows that leadership commitment is the single most important factor in determining whether TQM takes hold. When senior leaders visibly participate in improvement work, allocate resources to it, and hold themselves and their teams accountable for quality outcomes, TQM is more likely to produce lasting results.
5- Lean Methodology in Healthcare
Lean thinking originated in the Toyota Production System in post-war Japan and was brought to wider attention through James Womack and Daniel Jones's work on lean manufacturing in the 1990s. Its central idea is straightforward: define value from the perspective of the customer, map the process that delivers that value, identify and eliminate everything in the process that does not contribute to value, and then create a smooth and efficient flow of remaining activities. In healthcare, the customer is the patient, and value is defined by the care outcomes and experience they receive.
Lean healthcare identifies eight categories of waste that can accumulate in care delivery processes: overproduction, waiting, unnecessary motion, transportation, over-processing, inventory, defects, and underutilised people. These categories are known by the acronym DOWNTIME. A patient waiting for a bed that is already available, a clinician walking across a ward to collect supplies that should be at the point of care, a test being repeated because results were not communicated, a form being filled in twice because systems are not integrated, all of these represent waste in the Lean sense. Eliminating them improves efficiency and, critically in healthcare, reduces the opportunities for error and harm.
Research supports the effectiveness of Lean and related approaches in healthcare settings. According to a peer-reviewed study published in ScienceDirect, Lean Six Sigma tools have facilitated reductions in medical errors, waiting times, and costs of care delivery, while increasing patient satisfaction and patient turnover in hospitals applying these methods over two and a half decades in the United States.
6- Six Sigma in Healthcare
Six Sigma is a data-driven quality improvement methodology that focuses on reducing variation and defects in processes to a statistically defined level of performance. The name derives from the statistical concept of standard deviation: a Six Sigma process produces fewer than 3.4 defects per million opportunities, representing a near-zero rate of process failure. Originally developed by Motorola and popularised by General Electric, Six Sigma was introduced to healthcare in the late 1990s and has since been applied to a wide range of clinical and operational challenges.
The primary vehicle for Six Sigma improvement projects is the DMAIC framework: Define, Measure, Analyse, Improve, and Control. In the Define phase, the team specifies the problem, the goal, the process boundaries, and the patient impact. In the Measure phase, baseline data are collected to quantify the current level of process performance. In the Analyse phase, statistical tools are used to identify the root causes of defects or variation. In the Improve phase, solutions are designed and tested to address those root causes. In the Control phase, changes are standardised and monitoring systems are put in place to ensure that gains are sustained over time.
DMAIC Phase | Key Question | Common Healthcare Tools |
| Define | What is the problem and what does good look like? | Project charter, process map, Voice of the Patient |
| Measure | How bad is the problem and how do we know? | Data collection plans, baseline metrics, run charts |
| Analyse | What are the root causes? | Fishbone diagram, Pareto chart, statistical analysis |
| Improve | What changes will address the root causes? | Piloting solutions, PDSA cycles, simulation |
| Control | How do we sustain the improvement? | Control charts, standard operating procedures, dashboards |
Six Sigma is most effective where there is sufficient data, analytical capability, and process stability to support rigorous statistical analysis. It has been applied successfully to reducing hospital-acquired infection rates, decreasing medication dispensing errors, improving surgical instrument management, and shortening emergency department throughput times. A study published in the National Institutes of Health database found that applying Lean Six Sigma methodology to antimicrobial stewardship in a hospital in the UAE led to an 81.7% decrease in parenteral antimicrobial expenses and a 54.2% reduction in antimicrobial usage while clinical outcomes were maintained.
The DMAIC structure, for instance, can be used without the advanced statistical elements to provide a rigorous problem-solving framework. It is also worth noting that Six Sigma requires investment in training, particularly at the Green Belt and Black Belt levels for those leading projects, which is a resource consideration for budget-constrained organisations.

Working in the healthcare industry automatically means that you’re faced with an array of challenges. These could be related to processes and equipment or patient service and care. Healthcare is such a massive part of everyone’s life that we must focus on managing healthcare services
7- Lean Six Sigma: A Combined Approach
In practice, Lean and Six Sigma are increasingly applied together as a combined methodology known as Lean Six Sigma. While Lean focuses on eliminating waste and improving flow, Six Sigma focuses on reducing variation and defects. In many real-world quality problems in healthcare, both issues are present simultaneously: a care pathway may be inefficient because of unnecessary steps and also prone to error because of uncontrolled variation in how those steps are carried out. Lean Six Sigma addresses both dimensions in a single integrated approach.
Lean Six Sigma projects in healthcare typically follow the DMAIC structure while also employing Lean tools such as Value Stream Mapping and 5S at appropriate stages. The combination is powerful because it brings data rigour to Lean's process-thinking and brings operational efficiency consciousness to Six Sigma's analytical focus. For healthcare leaders, this means that improvement teams can address both the structural causes of poor quality, such as badly designed workflows, and the statistical causes, such as inconsistent clinical practice, within the same project.
The combined approach is also increasingly relevant in global health and NGO contexts, where organisations must simultaneously manage scarce resources efficiently and maintain consistent quality standards across diverse operational environments. Lean Six Sigma principles have been applied in humanitarian health logistics to reduce wastage of medical supplies, improve cold chain management for vaccines, and standardise clinical protocols across multi-country programmes. The key is keeping the application proportionate to organisational capacity.
8- ISO Standards and Quality Management Systems in Healthcare
The International Organisation for Standardisation has developed a family of standards that provide structured frameworks for quality management systems. The most widely applicable of these is ISO 9001, which sets out requirements for a quality management system based on seven principles: customer focus, leadership, engagement of people, process approach, improvement, evidence-based decision-making, and relationship management. ISO 9001 is not specific to healthcare, but its principles map closely onto the requirements of effective health service delivery, and it is used by hospitals, laboratories, pharmaceutical manufacturers, and health NGOs around the world.
ISO 9001 certification requires an organisation to document its key processes, establish quality objectives aligned with strategic goals, implement mechanisms for identifying nonconformities and corrective actions, conduct regular internal audits, and submit to external audit and certification by an accredited body. The certification process disciplines organisations to be systematic about quality and creates documented evidence that their management systems meet internationally recognised standards. This is particularly valued by donors, regulatory authorities, and government partners who need assurance about the quality of services they are funding or overseeing.
Framework | Primary Focus | Typical Application | Strengths | Limitations |
PDSA Cycle | Iterative testing of change | Clinical teams, ward-level improvement | Simple, fast, accessible | Can lack rigour if poorly applied |
TQM | Whole-organisation quality culture | Hospital management, NGO programme quality | Comprehensive, culture-building | Slow to embed, leadership-dependent |
Lean | Waste elimination and process flow | Operational efficiency, supply chains | Practical, frontline-driven | May overlook statistical variation |
Six Sigma | Defect and variation reduction | Complex processes with measurable defects | Rigorous, data-driven | Resource-intensive, requires training |
Lean Six Sigma | Combined efficiency and quality | Hospitals, multi-site health programmes | Broad applicability | Complex to implement fully |
ISO 9001 | Management system standards | Hospitals, laboratories, NGO health systems | Internationally recognised | Can become compliance-focused |
Beyond ISO 9001, healthcare-specific standards are also widely used. ISO 15189 covers quality management in medical laboratories. The International Society for Quality in Health Care oversees the ISQua accreditation framework, which is used to evaluate national hospital accreditation programmes. The Joint Commission International standard is another widely used accreditation framework for hospitals seeking international recognition. In humanitarian contexts, the Sphere Standards and the Core Humanitarian Standard provide quality benchmarks for health and humanitarian programmes, focusing particularly on accountability to affected populations, protection, and minimum standards of response.

The best quality management strategies encompass a multifaceted approach aimed at consistently delivering superior products or services that meet or exceed customer expectations. At its core, these strategies emphasise a commitment to continuous improvement, fostering a culture of quality throughout the organisation. Adopting international standards
9- Applying Quality Improvement in Public Health and NGO Settings
Quality improvement methodologies are not exclusively relevant to hospitals and clinical settings. Public health organisations and NGOs working in health programming face many of the same quality challenges, often in more complex and resource-constrained environments. The question of how to deliver consistent, evidence-based interventions across diverse communities, manage supply chains reliably, train and supervise field staff effectively, and use data to guide programme decisions is, at its core, a quality improvement question.
PDSA cycles are particularly well suited to NGO contexts because they can be run with minimal resources, adapted to local conditions, and used by teams with limited formal training in quality methods. An NGO implementing a community health worker programme can use PDSA cycles to test different approaches to supervision, community mobilisation, or data reporting, learn quickly what works in their specific context, and adapt accordingly. This is precisely the iterative, context-sensitive approach that development effectiveness literature increasingly argues is needed in complex settings.
10- Building a Culture of Quality: The Human Dimension
None of the methodologies discussed in this article will produce sustainable improvement without the right organisational culture. Culture in this context refers to the shared assumptions, values, and behaviours that determine how people actually work together on a day-to-day basis. A quality culture is one in which people at all levels feel psychologically safe to raise concerns about care, report errors without fear of blame, contribute improvement ideas, and take responsibility for the quality of their own work. Without this foundation, even the most sophisticated quality tools will produce limited results.
Creating a quality culture requires deliberate attention to leadership behaviour, communication practices, accountability systems, and the way errors and near-misses are handled. The concept of a just culture, developed within patient safety, provides a useful framework: a just culture distinguishes between blameless errors that arise from system failures and reckless behaviour that represents a genuine failure of individual responsibility, treating each differently and fairly. In a just culture, reporting is encouraged because it generates learning rather than punishment. Investigation of incidents focuses on system factors rather than individual blame. And improvement is understood as a collective responsibility rather than a management imposition.
Staff engagement is another critical factor. Quality improvement is most effective when the people who do the work are also those who design and test the improvements. Frontline clinicians, nurses, community health workers, and administrative staff have detailed knowledge of what causes delays, errors, and poor experiences in their specific environment. Methodologies that position them as improvement experts, rather than recipients of externally designed change, consistently produce better results. This requires investment in training, time for improvement work within normal working hours, and recognition of the contribution that quality improvement makes to professional development and organisational performance.
11- Measurement and Data in Quality Improvement
Quality improvement depends on measurement. Without data, it is impossible to know whether a problem exists, how significant it is, whether a change has made things better or worse, or whether an improvement has been sustained over time. Yet measurement in healthcare can be complex, resource-intensive, and contested. Clinicians sometimes resist measurement because they feel it misrepresents the complexity of their work. Managers sometimes focus on metrics that are easy to collect rather than those that are meaningful for patients. And in many low-resource settings, the basic data infrastructure needed for reliable measurement is either absent or unreliable.
Effective quality improvement measurement distinguishes between three types of measures: outcome measures, which capture the impact of care on the health and experience of patients; process measures, which track whether key activities in the care pathway are being performed correctly and consistently; and balancing measures, which check that improvements in one area are not causing problems elsewhere. Using all three types together gives a more complete picture of whether a change is genuinely an improvement.
Run charts and statistical process control charts are among the most useful measurement tools in quality improvement. Rather than comparing a single data point to a target, they display performance over time, making it possible to distinguish natural variation in a process from genuine signals that something has changed. This distinction is important because reacting to natural variation as if it were a signal can actually destabilise a process and make things worse, a problem known as tampering. In digital health environments, real-time dashboards increasingly make this kind of longitudinal monitoring accessible to frontline teams without requiring specialist statistical expertise.
12 - Challenges and Limitations of Quality Improvement Methodologies
Despite their proven value, quality improvement methodologies face a number of important challenges in practice. Sustainability is one of the most persistent. Improvement projects often produce short-term gains that erode over time when the project ends, staff change, or organisational attention moves elsewhere. Embedding changes into standard processes, updating training materials, revising protocols, and redesigning monitoring systems are all necessary to sustain gains, but they require ongoing effort and resources that organisations often struggle to maintain.
Scale-up is another challenge. A change that works well in a single ward, clinic, or programme may not transfer easily to a different context where patient mix, staff capability, physical environment, or organisational culture differs. Quality improvement science increasingly recognises that context matters profoundly and that improvement strategies must be adapted rather than simply replicated. This has implications for how NGOs and public health organisations manage quality across multi-site programmes, where standardisation and local adaptation must be carefully balanced.
The capacity gap is a further challenge, particularly in lower-income settings. Quality improvement requires people who have been trained in its methods and have protected time to apply them. In health systems facing staffing shortages, high turnover, and limited budgets for training and development, this can be difficult to sustain. Partnerships with academic institutions, international quality improvement networks, and specialist organisations can help bridge this gap, but they must be managed carefully to ensure that capacity genuinely transfers into the health system rather than remaining dependent on external expertise.
13 - Selecting the Right Methodology for Your Context
No single quality improvement methodology is right for every organisation or every problem. Selecting an approach requires honest assessment of the specific quality challenge being addressed, the organisational capacity and culture available to support improvement work, the resources, including time, people, and data, that can be committed, and the timescale within which improvement is needed. A simple PDSA cycle can produce meaningful change quickly with minimal resource, making it ideal for frontline teams addressing specific care gaps. TQM is better suited to organisations seeking to build long-term quality culture. Lean is most powerful where operational inefficiency and waste are the primary drivers of poor quality. Six Sigma is most appropriate where statistical precision is needed and analytical capacity exists.
In practice, the most effective quality improvement programmes combine elements from several methodologies. A healthcare organisation might use TQM principles to create the strategic direction and cultural conditions for improvement, Lean tools to map and redesign care pathways, PDSA cycles to test and iterate changes, and ISO standards to provide the governance framework and external accountability. Six Sigma techniques can be deployed for specific high-stakes problems where defect reduction demands rigorous analysis. This hybrid approach allows organisations to be pragmatic about what works in their context rather than being doctrinally committed to a single framework.
Conclusion
Healthcare quality improvement is a discipline that has matured considerably over the past three decades. The methodologies available today, from the iterative simplicity of the PDSA cycle to the analytical rigour of Six Sigma and the strategic breadth of TQM, provide healthcare organisations with a powerful and flexible toolkit for improving the safety, effectiveness, and efficiency of care. When applied thoughtfully, with attention to context, culture, and capacity, they produce real benefits for patients and communities.
The future of healthcare quality improvement lies in the combination of well-established methodologies with new enabling technologies, stronger cross-sector collaboration, and a deeper embedding of quality thinking into leadership practice and professional education. As health systems worldwide face growing demand, demographic pressure, and budgetary constraint, the ability to deliver consistently high-quality care will depend more than ever on organisations that treat improvement not as a project but as a permanent way of working.

Within the healthcare sector, it is essential to strongly focus on maintaining the highest standards of quality. As healthcare organisations directly impact patients' health, any situation where quality is lacking has the potential to cause significant harm. Many factors contribute to